.png)


This guide covers which markers to monitor, what your results mean, and how often to test.
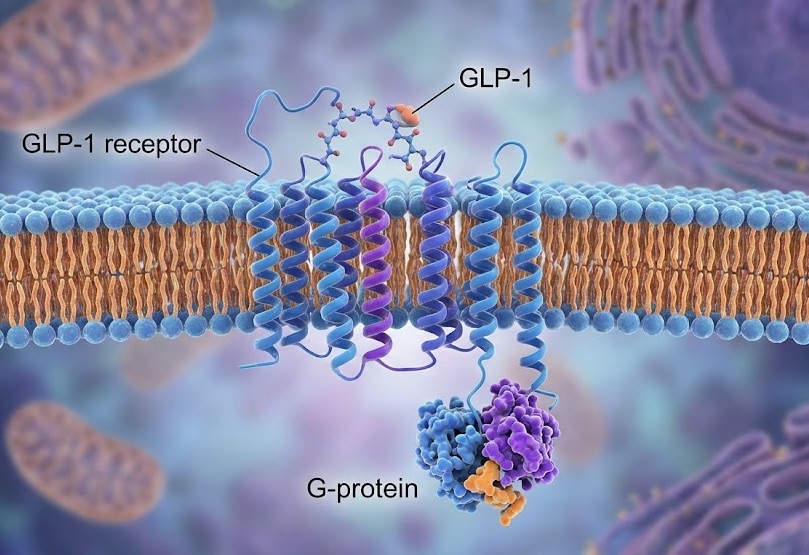
How GLP-1 Medications Affect Your Body
GLP-1 receptor agonists mimic a natural hormone called glucagon-like peptide-1. This hormone regulates blood sugar, slows stomach emptying, and signals fullness to your brain.
The medications work. Clinical trials like STEP 1 showed participants lost an average of 14.9% body weight over 68 weeks. The SELECT trial demonstrated a 20% reduction in major cardiovascular events.
But these are powerful drugs that interact with multiple organ systems.
What GLP-1s do in your body:
- Stimulate insulin release from pancreatic beta cells
- Slow gastric emptying, which reduces appetite
- Get metabolized primarily by the liver
- Are cleared partially through kidney function
- Have unknown long-term effects on thyroid C-cells
Nearly half of patients stop GLP-1 therapy within the first year. Many quit due to side effects that blood testing could have caught earlier. Markers like ALT, eGFR, and lipase reveal organ stress before you feel symptoms.
How Often Do You Actually Need Blood Tests on GLP-1 Medications?
In general:
- Baseline testing helps identify pre-existing issues before starting GLP-1 therapy
- Early follow-up (8–12 weeks) checks how your body is responding
- Ongoing testing may be spaced out or symptom-driven if results are stable and you feel well
Most clinicians prioritize trend analysis over isolated single results. A one-time fluctuation may not be meaningful, while consistent changes over time often provide a clearer picture of metabolic health.

The Organ Systems That Need Monitoring
Liver Function
Your liver processes GLP-1 medications. It's also where these drugs may provide unexpected benefits.
Research published in Frontiers in Endocrinology found that GLP-1 receptor agonists can improve liver health in people with metabolic dysfunction-associated steatotic liver disease (MASLD, formerly NAFLD). Semaglutide reduced liver fat, inflammation, and fibrosis scores in clinical trials.
But improvement isn't guaranteed. Your numbers confirm what's actually happening.
Key liver markers:
ALT is the most liver-specific. It rises early when liver cells become inflamed. AST increases with liver or muscle stress. GGT reflects bile duct function and oxidative stress.
The AST:ALT ratio helps identify causes. A ratio above 2 suggests alcohol-related liver stress. A ratio below 1 is typical of metabolic dysfunction-associated steatotic liver disease (MASLD, formerly NAFLD).
Alcohol and GLP-1 monitoring: Many people starting GLP-1 medications already have some degree of MASLD. Alcohol use compounds this. Even moderate drinking elevates GGT and can mask improvements from the medication. If you're working on reducing alcohol intake alongside GLP-1 therapy, tracking liver enzymes shows whether both efforts are paying off. For those dealing with alcohol use concerns, resources like Choose Your Horizon offer specialized support that complements metabolic health goals.
For a complete breakdown of these markers, see our guide to liver function testing. Individual marker deep-dives are available for ALT, AST, and GGT.
Kidney Function
GLP-1 medications can affect your kidneys. Dehydration is common on these drugs due to reduced appetite and GI side effects. Dehydration stresses kidney function.
The FDA prescribing information for semaglutide notes that acute kidney injury has been reported in patients taking GLP-1 receptor agonists. Most cases occurred in patients who experienced dehydration from GI side effects.
Key kidney markers:
eGFR below 60 ml/min indicates moderate kidney function loss. A drop of more than 15 points from your baseline warrants attention. Creatinine rising above reference ranges suggests reduced kidney function. Kidney health may be tracked at your annual physical if you get blood work done. Learn more about a comprehensive metabolic panel and what it typically includes.
Staying hydrated matters more on GLP-1 medications. So does monitoring.
Pancreatic Health
GLP-1 medications stimulate your pancreas to release insulin. That's their primary mechanism for blood sugar control.
The concern is pancreatitis. Acute pancreatitis has been reported in patients taking GLP-1 receptor agonists. The FDA label includes pancreatitis as a warning. Lipase is the primary marker to monitor. It is more specific to the pancreas than amylase and remains elevated longer after injury, making it the more reliable early warning signal. A rise above 3 times the upper limit of normal - particularly alongside upper abdominal pain that radiates to the back — requires immediate clinical evaluation.
Key pancreatic markers:
Both amylase and lipase can rise modestly on GLP-1 medications without indicating pancreatitis — this is a known pharmacological effect. What matters is the magnitude of the rise and whether it's accompanied by symptoms. For a full breakdown of what amylase levels mean, normal ranges, and how to interpret results alongside lipase, see our guide to amylase blood test results and what they indicate.
Blood Sugar Control
The primary purpose of GLP-1 medications is improving blood sugar. Testing confirms whether the medication works for you.
Key metabolic markers:
HbA1c is the more reliable indicator. It reflects long-term blood sugar control rather than a single moment. If HbA1c doesn't improve after 3 months on medication, dosing or approach may need adjustment.
The connection between blood sugar and liver health runs deep. Insulin resistance affects both systems. Our guide on insulin resistance and liver health explains this relationship.
Cardiovascular Markers
GLP-1 medications have demonstrated cardiovascular benefits in clinical trials. The SELECT trial showed significant reduction in heart attacks, strokes, and cardiovascular death.
Advanced testing tracks whether you're experiencing these benefits.
Key cardiovascular markers:
Weight loss alone improves most cardiovascular markers. ApoB in particular is worth tracking — it's a more direct measure of cardiovascular risk than standard LDL.Testing shows how much improvement you're actually getting.
Thyroid Function
The FDA label for semaglutide includes a black box warning about thyroid C-cell tumors, based on animal studies. The clinical significance in humans remains under investigation, but it's why thyroid monitoring is worth including in your baseline and annual testing.
GLP-1 receptors are present in thyroid tissue. Rapid weight loss can also independently affect thyroid hormone levels, making it difficult to distinguish medication effects from weight-loss effects without baseline data.
TSH outside the 0.5–4.5 range warrants follow-up. Hypothyroidism (high TSH) can cause fatigue and slow metabolism — symptoms that overlap significantly with GLP-1 side effects, making baseline data particularly useful for distinguishing the cause.
Thyroid testing is not required for everyone on GLP-1 therapy. It is worth prioritizing if you have a personal or family history of thyroid disease, experience unexplained fatigue, or notice changes in heart rate or body temperature regulation.
What Changes to Watch For
Not every fluctuation matters. Here's what does:
Share significant changes with your prescribing clinician. Single elevated readings may not indicate problems. Trends over multiple tests reveal the real picture.
GLP-1 Monitoring for Diabetes vs. Weight Loss: What’s Different?
Not everyone takes GLP-1 medications for the same reason, and monitoring needs differ.
If you’re using GLP-1s for diabetes management:
- HbA1c and fasting glucose are primary markers
- Kidney function is monitored more closely, especially if you take metformin or insulin
- Lipids help track cardiovascular risk
If you’re using GLP-1s primarily for weight loss:
- Baseline metabolic labs still matter
- Liver enzymes and kidney function help track safety
- Blood sugar markers may be checked less frequently if you don’t have diabetes
In both cases, testing is most useful because it informs decisions, and empowers the user to own their health.
GLP-1s and Muscle Mass
Rapid weight loss does not only reduce fat mass — it can also reduce lean muscle mass if protein intake and resistance training are inadequate.
Preserving muscle mass during GLP-1 therapy is important for:
- metabolic health
- insulin sensitivity
- long-term weight maintenance
- strength and mobility
Key considerations:
- prioritize adequate protein intake
- incorporate resistance training
- avoid excessively aggressive calorie restriction
Muscle loss can also affect lab interpretation. Creatinine levels may decline alongside reductions in muscle mass, which can complicate kidney marker interpretation over time.
Don’t Overlook Electrolytes
Dehydration is one of the most common side effects of GLP-1 medications, especially early in treatment.
Reduced fluid intake, nausea, or vomiting can lead to electrolyte imbalances, including:
- Sodium
- Potassium
- Chloride
Electrolyte shifts can worsen fatigue, dizziness, muscle cramps, and kidney stress. In people with symptoms or rapid weight loss, electrolyte testing can provide useful context alongside creatinine and eGFR.
Nutrient Levels to Consider During GLP-1 Weight Loss
Significant appetite reduction and rapid weight loss can affect nutrient intake over time.
While GLP-1 medications don’t directly deplete nutrients, people eating less may develop low or borderline levels, particularly:
- Vitamin B12 (especially if also taking metformin)
- Vitamin D
- Iron (especially in menstruating women)
These labs aren’t required for everyone. But if you experience fatigue, hair loss, dizziness, or prolonged reduced intake, testing can help identify correctable deficiencies.
When and How Often to Test
Healthcare providers recommend baseline testing before starting GLP-1 therapy. Then periodic monitoring during treatment.
Before starting: Get a baseline panel covering liver, kidney, pancreatic, thyroid, and metabolic markers. This gives you a reference point for all future comparisons.
First 3 months: Test at 6-8 weeks. This catches early organ stress while your body adjusts to the medication. Side effects are most common during titration.
Ongoing monitoring: Every 3-6 months depending on your health status. More frequent testing makes sense if you have pre-existing conditions or experience side effects.
If symptoms appear: Test promptly for persistent abdominal pain (pancreatitis concern), unusual fatigue (liver or thyroid), swelling or changes in urination (kidney), or rapid heart rate (thyroid).
If you are curious about how GLP-1s impact women in particular, you can dive deeper on our sex-specific guide, to see unique considerations.
What Testing Reveals Over Time
Single snapshots miss the full picture. Patterns across multiple tests show how your body actually responds to GLP-1 therapy.
Testing reveals:
- Whether your liver is improving, stable, or stressed
- If kidney function remains stable during treatment
- Whether blood sugar goals are being met
- If cardiovascular risk markers are improving
- Any early warning signs before symptoms appear
Many people feel better on GLP-1 medications before their lab markers normalize. Others see lab improvements before noticing physical changes. Testing shows what's happening at the cellular level.
The goal isn't perfect numbers on every test. It's understanding your trajectory. Consistent improvement over 6-12 months matters more than any single result.